Case Study · AI Enablement · Healthcare Patient Access
The 15-minute referral.
A healthcare patient-access company whose platform turns physician referrals into confirmed appointments — except every referral first had to be manually transcribed between systems: a measured ~15 minutes of read, interpret, verify, and re-key across four screens. The fix wasn’t OCR. It was structure, verification, and an audit trail — built under the governance healthcare actually demands. The system we designed is being built by their own team, to expectations we set together: person-to-person calling down ~97%, and daily call capacity up from 400 human-dialed calls to 5,000 AI-automated interactions.
The company
A real platform with a manual front door.
Built by operators, serving major health systems, with a genuine platform behind it — this is not a laggard. But the front door of the whole operation was human: referrals arrive from hospital EHRs, and an operator reads each one, interprets it, verifies it across systems, and re-keys it into the platform. We didn’t take anyone’s word for the pain — we got operator access and walked a live referral ourselves: ~15 minutes. And the time isn’t typing. It’s reading, interpreting, and verifying across four different systems.
Multiply that by every referral, every clinic, every day — while half the industry’s specialty referrals never get scheduled at all — and the front door is the business case.
The reframe
Structure, not OCR.
The obvious pitch was “point AI vision at the documents.” We killed that framing early. The leverage isn’t reading pixels — it’s the mapping layer: one canonical field schema every referral lands in, no matter how it arrives. So intake became a ladder:
Under all three tiers, the same pipeline — exception-based by design:
The engagement so far
Measured, mapped, governed, taught.
Measured the floor ourselves
Hands-on operator access, a live referral walked end to end, a stopwatch on every step. Baseline before AI touches anything — when the numbers land, nobody has to take them on faith.
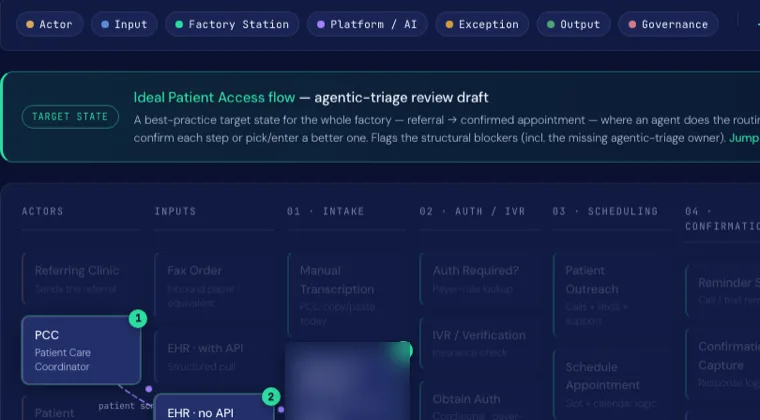
✓ ~15 min/referral, measuredMapped the whole factory
Intake → authorization → scheduling → confirmation, as one interactive systems map with live queue depths per station. Two competing internal process maps — operations’ and product’s — reconciled into a single canonical view of how work actually moves.
Shipped a working proof, not a deck
A live extraction service against a public federal provider registry — real lookups, mapped into the canonical schema, zero protected data — handed to their engineering team as running code plus an engineering-handoff page: field maps, pipeline, open questions, guardrails.
✓ Live · handed to engineeringInstalled the governance the domain demands
Protected data moves only through covered, compliant endpoints — never consumer AI tools. No auto-commit: humans approve before anything writes. Full audit trail: source, confidence, reviewer, final record. We advise; the client owns deployment and compliance sign-off.
Taught leaders first, then the floor
A live build demo for the executive team, then an open AI education forum for everyone. Education-first is the strategy: the tools change monthly; a team that understands the principles doesn’t.
Grew a champion — the real deliverable
Months in, their own senior engineer presented AI dev practices to the whole team — plan-first-then-code, grounding agents in the repo, forcing verification — our guidance, contextualized to their systems, in his voice. Adoption that doesn’t depend on us being in the room.
✓ Champion teaching, unpromptedThe results
What we set in motion.
The structural work was delivered and handed over: the baseline measured, the architecture agreed, a working proof placed in their engineers’ hands, the governance installed, and their own champion teaching the practices onward. The capacity numbers below are the expectations we set with the client — and the measured 15-minute baseline is what they’ll be judged against.
Why it’s built this way
Measure it yourself
We don’t baseline from interviews. Operator access, a live walkthrough, a stopwatch — then the improvement claim can survive an audit.
Schema is the product
The canonical field mapping outlives any OCR model, any vendor, any tier. Structure first; extraction is a detail.
Humans on exceptions
Automation earns trust by handling the routine and escalating the ambiguous. Nothing writes without a person or a proof.
Champions over consultants
The engagement succeeds when their people teach it without us. That’s the deliverable the invoice never quite captures.
What you get
What a patient-access engagement ships — structure, not just OCR.
- Discovery with a measured baseline — the ~15-minute referral was timed, not guessed
- The ideal-state intake flow — every station mapped, agentic triage marked (artifact at right)
- A 3-tier intake ladder — API ingestion → structured portal → OCR with human review
- Exception-based review design — humans handle the fallout lane, not the routine
- Healthcare-grade governance — PHI boundaries, human-in-the-loop, full audit trail
- An expected-impact model with honesty labels — expected, clearly marked, never promised
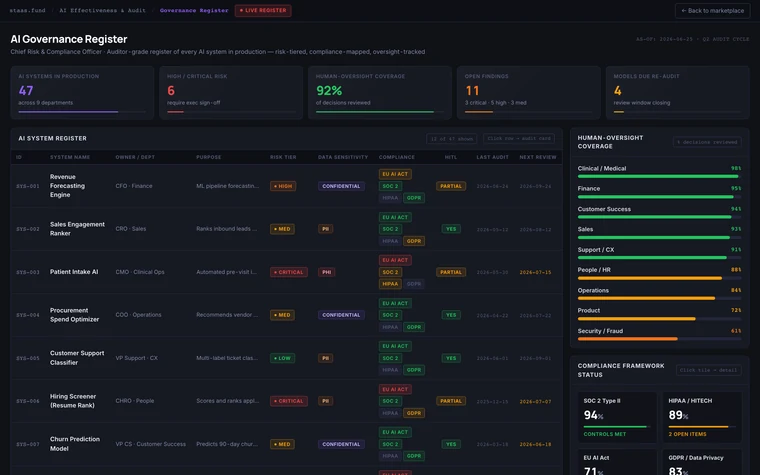
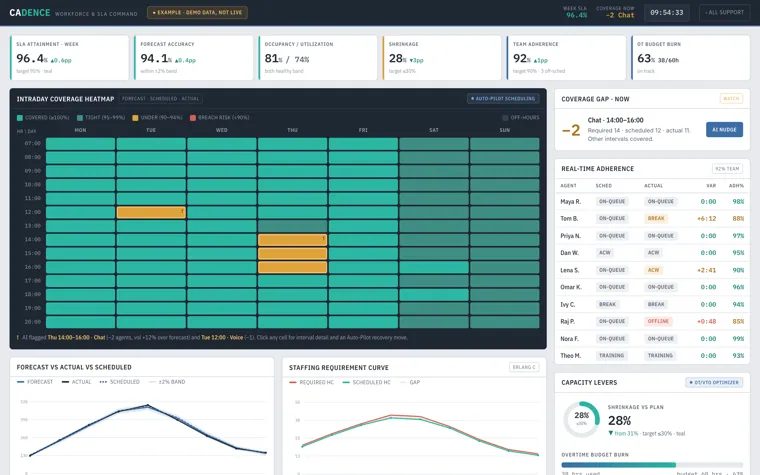
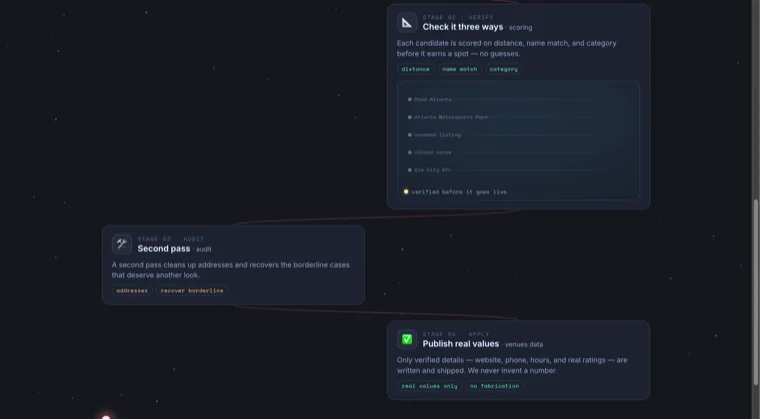
Representative artifacts — a real process review, our own production pipeline, dashboards from our 44-dashboard marketplace. Client identifiers removed. Your versions get built on your systems.
See where you stand
Before you automate intake, is your data ready? Score your data layer first.
Regulated industry, manual front door?
Healthcare, finance, anywhere the data is protected and the stakes are real — we build AI systems with the governance your auditors expect and the baselines your board can trust.
Start a conversation → More case studies